Pain Tutorial
Ascending and descending pathways of the spinal cord
Case Report
Case History
A woman aged 56 presented with interscapular pain which had been increasing for two weeks and was keeping her awake at night. Her left leg had begun to give way. When she took a bath the previous night she could not feel the temperature of the bath water with her right foot. Two years earlier she had had a carcinoma excised from her left breast.
Examination
The patient was lying, still distressed by pain centred on the spine of the 6th thoracic vertebra , which was slightly tender. There was no wasting or fasciculation of her leg muscles. The left leg was slightly spastic . There was slight weakness of the left hip, knee and ankle. The left knee and ankle reflexes were increased and the left plantar response was extensor (Babinski sign ). Pain and temperature sensation were impaired on the right in all regions below the 8th thoracic dermatome . Vibration sensation was absent at the left ankle. She could stand and walk only with difficulty because of pain, and dragged her left foot.
Management
radiographs showed a collapse of the 6th thoracic vertebra. An urgent magnetic resonance scan showed a mass compressing the anterolateral aspect of the spinal cord on the left side at that level. A neurosurgeon advised against surgery. A radiotherapist started urgent radiotherapy to the 6th thoracic vertebra and oral steroid treatment. Within 2 days her pain was relieved and within a week she was able to walk more easily.
Radiographs
Click each of the radiograph thumbnail images below to reveal a larger version with a description. Note that the radiographs below are not from the person described in the case above but show similar, albeit more severe, compression of the spinal cord at T6 produced by a tumor.
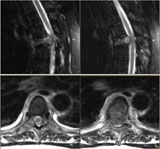
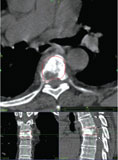
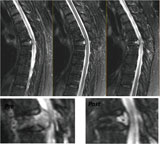


. Pre- and post comparison (insert), dramatically demonstrates the benefits of this radiosurgical procedure in this case.")