Marjorie Williams
78, Female
Click on the tabs below to view the results and interpretation of these investigations.
Haematology
Haemoglobin (Hb)
Hb 130 g/L. (130-180)
This is at the lower end of the normal range and suggests that Mrs Williams does not have chronic kidney or inflammatory disease.
White cell count
WCC 14 x109/L (3.6-11.0).
This is raised in keeping with infection.
Clinical Biochemistry
Urea
28 mmol/L i(2.5-7.8). This is high in keeping with dehydration and renal impairment.Creatinine
252 µmol/L (70-110). This is high in keeping with renal impairment. It is not possible to tell if this represents acute kidney injury (AKI) or chronic kidney disease (CKD) without knowing previous measurements. This level of creatinine gives her an estimated glomerular filtration rate (eGFR) of 17 ml/min (MDRD equation).
Potassium
Potassium 5.2 mmol/L (3.5-5.0). This is high and is in keeping with renal impairment.
Arterial blood gases
On room air:
- pH 7.28 (7.35 to 7.45)
- pO2 10.9 kPa (>10.7 on room air)
- pCO2 3.2 kPa (4.7 to 6)
- HCO3 15 mEq/L (21 to 27)
- Base excess -8 (-2 - +2)
- Oxygen saturation 97%
Imaging
Ultrasound of the kidneys and bladder
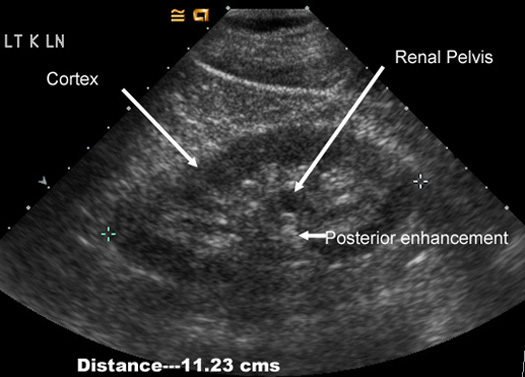
Both kidneys appear to be normal in size, shape, and position. The left kidney is 10.2 cm and the right kidney is 10.9 cm (normal 10-13 cm). There is slight loss of corticomeduallary differentiation in keeping with medical causes of kidney disease. There is no hydronephrosis. The bladder could not be examined as it was empty at the time of scanning.
This result rules out obstruction as the cause of renal impairment. It also suggests that the renal impairment is acute as the kidney sizes are normal. In chronic kidney disease, the kidneys usually reduce in size. Loss of corticomeduallry differentiation means that it is difficult to tell on the scan where the cortex finishes and the medulla starts (this is normally quite easy to see). This picture occurs with many causes of kidney injury and is non-specific.

Ultrasound of a kidney showing loss of corticomedullary differentiation
Ultrasound of a normal kidney
Chest X-Ray
Mrs Williams’ CXR is normal suggesting the cause of her sepsis is unlikely to be pneumonia
Electrocardiogram
Her ECG shows sinus tachycardia with no evidence of acute ischaemia.
Immunology
Acute screen
- Autoantibodies: Negative
- Anti-nuclear factor: Negative
- Anti-neutrophil cytoplasmic antibody: Negative
- Anti glomerular basement membrane antibody: Negative
- Serum protein electrophoresis and urine free light chains: Normal
These results suggest that the cause of Mrs Williams' kidney injury is unlikely to be autoimmune (e.g. systemic lupus erythematosus, ANCA positive vasculitis, Anti-Glomerular basement membrane disease) or secondary to myeloma (no paraprotein or abnormal light chain production).