Coronary Artery Disease (CAD) and Ischaemic Heart Disease (IHD)
- Coronary artery disease (CAD)
- Events in CAD
- Ischaemic Heart Disease (IHD)
- Pathology of myocardial ischaemia/infacrtion
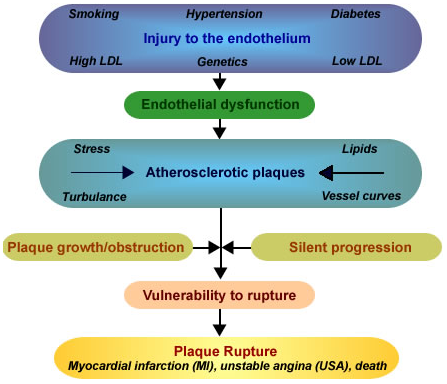
Risk factors of CAD (1)
Independent risk factors are:
- Hypercholesterolemia
- Smoking
- Hypertension
- Hyperglycemia/diabetes mellitus or otherwise
- Hereditary differences (homocysteine processing/metabolism, etc.)
Indirect risk factors (significant) are:
- Stress
- Diet rich in saturated fats
- Lack of exercise
- Obesity
- Diet low in antioxidants
- Men or women over 65
Coronary artery disease (CAD) is the end result of the accumulation of atheromatous plaques within the walls of the arteries that supply the myocardium.
It is the most common form of heart disease and is due to atherosclerosis, in which arteries become narrow and hardened. CAD ultimately leads to myocardial ischaemia, myocardial infarction or heart failure and at times to sudden death.
In CAD, myocardial ischaemia occurs as a result of coronary spasm and obstruction. Clinically, it is manifested as angina pectoris (with or without ECG changes).
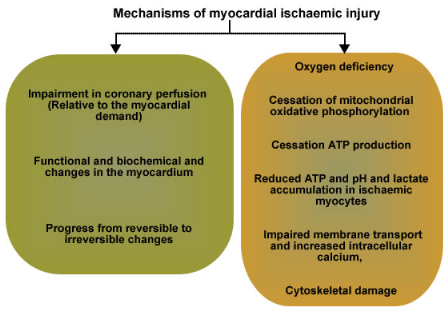
Mechanisms of myocardial ischaemic injury
Ischaemic heart disease (IHD) is a group of closely related syndromes/conditions resulting from reduced blood supply to the heart. In general, these may be expressed as any one of the following clinical syndromes:
- Acute myocardial infarction (AMI - see below)
- Angina pectoris
- Chronic ischemic heart disease
- Sudden cardiac death
AMI |
|
Symptoms of AMI: |
|
Chest pain with greater severity and of duration (over 30 minutes) than angina
|
Signs of AMI:
|
Patterns of myocardial infarction
Subendocardial infarcts affect the inner third or half of the left ventricular wall (diffuse or multi-focal and patchy in distribution)
Transmural infarcts involve the entire thickness of the left ventricular wall (are usually regional)
Myocardial infarction (MI) usually results from the sudden occlusion of a coronary artery when a plaque ruptures, activating the clotting system and atheroma-clot interaction fills the lumen of the artery to the point of sudden closure. (1)
Myocardial infarction is characterised by necrosis of myocytes due to ischaemia and begins in the subendocardium as blood flow in the myocardium occurs inwards from the epicardium to the endocardium. It progresses from the subendocardium to the supepicardium over a time. Ischemic changes may be focal or diffuse.