3: Introduction to the Analytical Tool
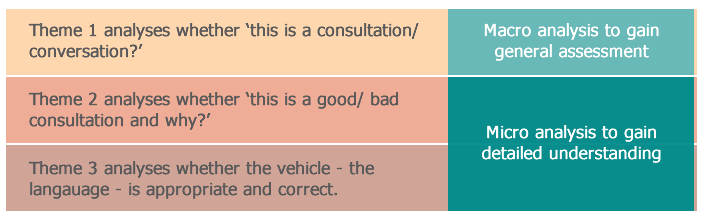
3.2 Three Themes
Click on the tabs below to see each area.
The following reflective questions will help you use Theme 1 for analysis:
- a] Turn-taking
- Did the doctor identify the right place to pass the turn to patient as well as taking over from the patient?
- To avoid overlap, which may discourage patient to disclose difficult information.
- To take turns back when necessary.
- To avoid overlap, which may discourage patient to disclose difficult information.
- Did the doctor identify the right length of turns?
- Has the Dr been talking too much or too little?
- Has the patient been talking too much or too little that the Dr needs to support?
- Has the Dr been talking too much or too little?
- Did the doctor identify the right place to pass the turn to patient as well as taking over from the patient?
- b] Co-construction
- Has the doctor encouraged and facilitated patient’s participation/co-construction?
- Has the doctor adapted to Pt's preferred communication style?
- Has the doctor negotiated for understanding?
- Has the doctor encouraged and facilitated patient’s participation/co-construction?
- c] Recipient design
- Is what the doctor says in response to what the patient is saying?
- Has the doctor taken patient’s words on board?
If these are failed, the consultation is highly likely to be unsuccessful.
Theme 1 analyses whether a consultation is constructed as an interactional conversation. To further analyse how the interaction has been conducted and whether the interactions are successful we need to go deeper to analyse Themes 2 and 3.
Click on the next tab above to continue.
Note: Click on the panels below to view the hide/ show the themes.
- Contextualization cues signal:
- what the activity is,
- how semantic content is to be understood and
- how each sentence relates to what precedes or follows". It is up to the listener to pick these up accurately and to respond accordingly.
- Framing is an inevitable process during which we put things into context. It can be situational context or topical context, either abstract or specific. Below shows the types of frames in a consultation.
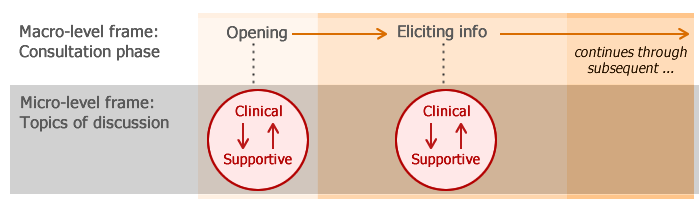
Types of Frames
- Positioning indicates the view point from which people interpret as well as produce meanings in a conversation. Positioning usually changes as people refer to their different social and conversational roles. Apart from being a patient, patients’ social roles may also include being a mother, daughter, sister, lawyer, etc. Conversationally a patient can be a listener, a speaker, an eavesdropper, etc. The same is true to the doctors. All these roles may become relevant to a consultation and affect the way people make sense of and for each other. Improving awareness of students’ own positioning may also help you to relate your own experience with that of the patient, which can help achieve empathy.
- Social Action: Conversation is the way we perform social actions (eg. asking a question, clarifying a misunderstanding, restoring rapport, negotiating, diagnosing) in order to fulfil certain social functions (eg. providing care for patient, or seeking healthcare). The doctor’s actions may include: building rapport, eliciting information, facilitating information giving, empathising, comforting, counselling, discussing, negotiating, diagnosing and treating. The patient’s actions may include: giving and seeking information, seeking emotional support, discussing and negotiating.
For further details in the meaning of these word, please see pages 12-17 in the handbook.
- Identify the contextualisation cues of both the doctor and the patient
- Distinguish the frames that the contextualisation cues signal (e.g. various phases of the consultation, clinical topic or supportive topic)
- Examine the positions/roles that the participants take in the frames
- Analyse the actions embodied in the participants’ language (e.g. advice giving, building rapport)
- Confirm how the overall meaning is evident in the interaction
- note that meaning of actions is the meaning understood by the participants which is manifested in the interaction;
- You are analysing how the participants understand each other’s meanings not how you understand the meanings.
- There is a difference between your meaning and participants’ meaning although they may overlap, if you analyse correctly.
- Meaning confirmed in interaction is an objective understanding of the communication between the participants.
Click on the next tab above to continue.
English is the language used in conducting most consultations in the UK. Knowing its linguistic features, such as the principles of politeness and grammatical structures can help us analyse the language when used in interaction. We will introduce you two more generic concepts before we discuss the grammar, which some people may already be familiar.
- Register is “a stylistic variant of a language appropriate to a particular social setting...” (Fromkin and Rodman, 1998: 535). A clinical encounter is both a mixture of institutional and mundane talk and a mixture of high formal and low informal registers. However, one would avoid very informal language (e.g. swearing, certain forms of slang), and very formal language (e.g. Latin words or other words particular to medical professionals). It is very likely one would use a lower register to talk to a patient; however, a well-informed patient may prefer to use a higher register.
- Facework has to do with the social image a person presents and/or is thought to present to another during conversation. It can only be determined by a fellow speaker. In reality, a person is constantly working to project a positive face as well as helping others to maintain their own face, hence the term “facework”. By definition, “the term face may be defined as the positive social value a person effectively claims for himself …during a particular contact [with others]” (Goffman, 1955: 213). It is something that is emotionally invested, and that can be lost, maintained, or enhanced, and must be constantly attended to in interaction. In general, people cooperate (and assume each other's cooperation) in maintaining face in interaction, such cooperation being based on the mutual vulnerability of face (Brown and Levinson, 1987). One can also be said to “save face” for themselves or their interactants, and it is an important part of maintaining positive social relations (i.e. to avoid conflict). Saving face is often achieved through politeness maxims (see below).
Politeness: You are probably familiar with the notion of being polite. But do you know there are two types of politeness, each with a set of subsequent strategies in the English language?
- Negative politeness: Makes a request less infringing, such as "If you don't mind..." or "If it isn't too much trouble..."; it respects a person's right to act freely. In other words, deference.
- Positive politeness: Seeks to establish a positive relationship between parties; respects a person's need to be liked and understood.