Cardiac chest pain
Angina pectoris refers to discomfort or pain associated with an imbalance between myocardial oxygen supply and demand, generally due to a critical stenosis of an epicardial artery. Associated symptoms include diaphoresis (excessive sweating), nausea, vomiting, and weakness. Chest pain and diaphoresis are the two most common symptoms of acute myocardial infarction (MI). The Levine sign, which is the patient placing a clenched fist on the sternum when describing his or her chest pain, may also be an indication of ischaemic pain.
Typical symptoms, based on the common presentation in men, include a crushing, pressure, or squeezing sensation in the centre of the chest that may or may not be described as pain. *Pain is commonly referred to the left shoulder and flexor portion of the left arm.
It is important to recognise that there is great variability in the location of cardiac pain among different patients and with the associated subjective sensations. For example, anginal pain may less commonly radiate to the right arm, neck, or jaw, or in the epigastric region. Not all patients describe typical “crushing pain”, but instead may describe a fullness sensation or a sharp, stabbing, burning pain. This “atypical” chest pain may be misinterpreted, for example as being the result of gastro-oesophageal reflux. Episodes of myocardial ischemia can also occur in the absence of chest pain. “Silent myocardial infarction” is more common in patients with diabetes mellitus, for example.
Referred pain
*Referred pain is pain localised to a body part other than the site of the painful stimulus. For example, myocardial ischaemia causing pain localised to the left upper arm.
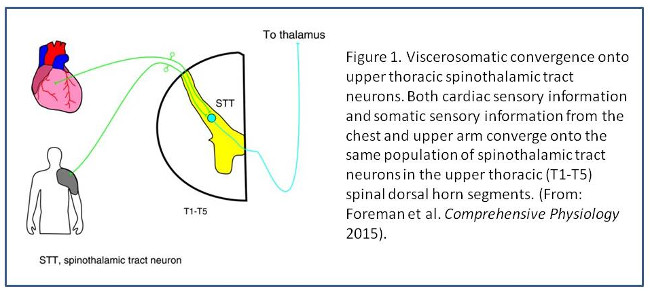
The convergence projection theory (Ruch 1961) sought to explain how pain originating from a visceral organ could be referred to somatic structures. In essence, this theory states that visceral and somatic noxious sensory inputs converge onto a common pool of projection neurons, such as spinothalamic tract neurons, within the central nervous system (Figure 1). These projection neurons usually transmit noxious somatic input to higher brain centres, where the input is interpreted as somatic pain localised to that somatic body part. Some pools of projection neurons are “shared” by sensory nerves innervating visceral and somatic body parts. For example, cardiac sensory information and somatic sensory information from the chest and upper left arm may converge onto the same population of spinothalamic tract neurons in the upper thoracic (T1-T5) spinal dorsal horn segments (Figure 1). In this case, the convergence projection theory postulates that noxious cardiac stimuli, such as myocardial ischaemia, will result in the brain localising that painful stimulus to the upper left arm.
The complexity and inter-individual variability in convergence of somatic and visceral information likely explains the great variability in sensations reported by patients with myocardial ischaemia (Foreman et al. Comprehensive Physiology 2015).
[SOURCE:Foreman et al. Comprehensive Physiology 2015]