
Bashir Agim
75, Male
The main findings on examination indicate the following:
-
Tachycardia and hypotension:
-
Corneal arcus
-
Xanthelasma
-
Tendon xanthoma
-
Epigastric and left sided abdominal tenderness with guarding
-
Urinalysis
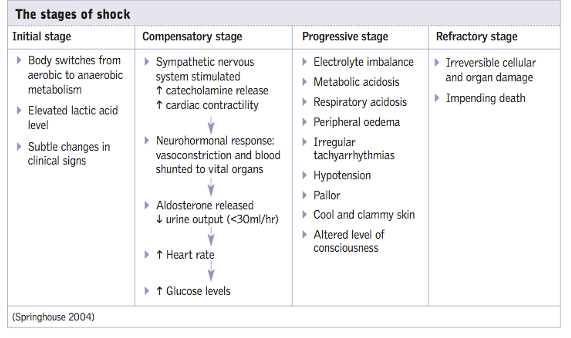
The tachycardia is almost certainly the result of activation of the sympathetic nervous system. This has also caused peripheral vasoconstriction and sweating, giving rise to the cold and clammy hands. It is likely that the sympathetic nervous system has been activated by a reduction in cardiac output and the consequent low blood pressure. The fact that the blood pressure remains low despite the tachycardia and peripheral vasoconstriction suggests that despite compensatory mechanisms, organ perfusion is compromised. The stages of shock are illustrated below:
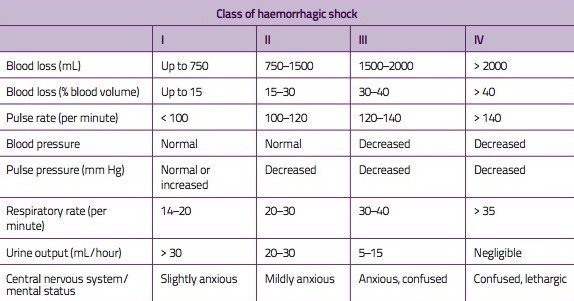
It is useful to know the different classes of haemorrhagic shock so that one can identify which stage of shock your patient may be in and how aggressive resuscitation will need to be to replace the lost volume of blood. This is illustrated in the table below:
The presence of a corneal arcus, xanthelasma and tendon xanthoma suggest hypercholesterolaemia. The tendon xanthoma (typically affecting the extensor tendons on the hands and the Achilles tendons) are virtually pathognomonic of familial hypercholesterolaemia (FH).
This indicates that there is likely to be an abdominal source of pathology that is causing this presentation. Guarding is a protective phenomenon whereby the abdominal muscles increase their tone when an area is palpated which has underlying inflammation. Peritonism is caused by inflammation of the peritoneum caused by organ inflammation or viscus perforation. Of note, in elderly patients guarding may not be present as they lose their muscle bulk with age. Hence, the absence of guarding or peritonism in the elderly does not necessarily mean that there is no underlying pathology.
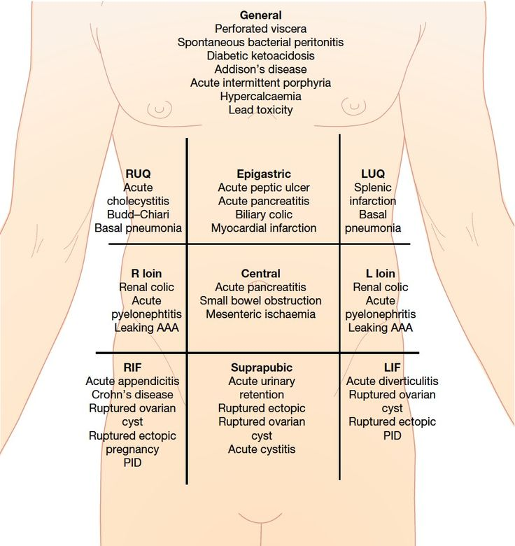
[SOURCE: https://anatomyofdiagram.com/abdominal-quadrants-and-their-organs/abdominal-quadrants-and-their-organs-acute-abdominal-pain-and-starting-ddxquadrant-doctor-stuff/]
The presence of blood on a urine dipstick can have several causes including UTI, renal stones, pyelonephritis, malignancy of the renal tract. It is important to note that microscopic haematuria can also arise from inflammation within structures that lie next to the renal tract/ureter such as diverticulitis and an AAA.