
Bashir Agim
75, Male
Click on the tabs below (and click headings to open and close the subpanels) to view the results and interpretation of the investigations.
12 lead ECG
Explanation:
The presence of ST elevation indicates that an epicardial coronary artery has occluded and urgently needs to be opened. If the ECG is normal it should be repeated after 10 minutes. If changes are present on the ECG other than the ST elevation, a patient may still be having an MI but the advantages of immediate reperfusion are less well proven.
In practice, a patient admitted with a possible MI would have continuous ECG monitoring; this will indicate any disturbances of rhythm but a full 12 lead ECG is required for diagnosis.
Elecrolytes, urea, creatinine
Explanation:
Renal pathology may be accompanied by abnormal renal function results.
Results
| Investigation Name | Investigation Result | Normal Range | Units |
|---|---|---|---|
| Sodium | 141 | 137 - 145 | mmol/L |
| Potassium | 4.2 | 3.5 - 4.9 | mmol/L |
| Urea | 4.5 | 2.5 - 7.5 | mmol/L |
| Creatinine | 97 | 60 - 110 | µmol/L |
Glucose
Explanation:
If it is raised, it may indicate previous diabetes in which case the glycosylated-haemoglobin will also be abnormal (reflecting glucose levels over the last two months) Alternatively it can be raised as part of the “stress response”.
Results
| Investigation Name | Investigation Result | Normal Range | Units |
|---|---|---|---|
| Glucose | 14 | Random < 11 | mmol/L |
| Glycosylated Haemoglobin | 5.2 | < 6 | % |
The glucose concentration is elevated; this is typical of a stress response, with catecholamine release leading to glycogenolysis. The normal HbA1c suggests that the patient does not have diabetes.
Cholesterol
Explanation:
If this is taken within the first few hours of symptoms, it is likely to reflect the cholesterol before acute presentation. In addition, it is worth measuring low density lipoprotein (LDL) and high density lipoprotein (HDL).
Results
| Investigation Name | Investigation Result | Normal Range | Units |
|---|---|---|---|
| Total Cholesterol | 8.2 | < 5 | mmol/L |
Note that since there is a continuous association between cardiovascular risk and total and LDL cholesterol concentrations, extending to total cholesterol concentrations even below 5mmol/L, it is inappropriate to use the term ‘normal’ value. It is more relevant to consider ‘ideal’ values or targets for treatment.
Arterial blood gas
Explanation:
Arterial blood gases will document whether oxygenation is impaired. This is particularly important if pulse oximetry suggest that saturation is lower than 93%. In addition, the low blood pressure and tachycardia suggest organ perfusion is compromised and this can be documented by measuring the base excess.
Results
| Investigation Name | Investigation Result | Normal Range | Units |
|---|---|---|---|
| PaO2 (breathing air) | 8.0 | 11.0 - 13.5 | kPa |
| PaCO2 | 4.0 | 4.8 - 5.6 | kPa |
| pH | 7.20 | 7.35 - 7.45 | |
| HCO3 | 18 | 22 - 26 | mmol/L |
| Lac | 5 | < 2 | mmol/L |
| BE | -2 | -2 to +2 |
Creatine kinase and troponin
Explanation:
Creatine kinase and troponin are intracellular proteins released from dead heart muscle cells. Creatine kinase exists in a variety of cells particularly skeletal muscle and so is now rarely used to diagnose myocardial infarction. Troponins I and T are specific to cardiac muscle and are the favoured biomarkers to diagnose myocardial infarction and also other forms of myocardial injury. Creatine kinase rises rapidly and within 4 to 6 hours of the onset of myocardial infarction. Creatine kinase is therefore useful in the early diagnosis of possible cardiac damage. Troponins rise more slowly and after 3 to 6 hours. However, their release is specific. The presence of troponin release together with chest pain is diagnostic of acute myocardial infarction. The maximum amount of creatine kinase release and troponin release is related to the volume of cardiac muscle that has infarcted.
Liver function tests
Results
| Investigation Name | Investigation Result | Normal Range | Units |
|---|---|---|---|
| Protein | 72 | 61 - 76 | g/L |
| Albumin | 41 | 37 - 49 | g/L |
| Bilirubin | 19 | < 22 | µmol/L |
| Alaninine aminotransferase | 29 | 1 - 31 | U/L |
| Alkaline phosphatase | 62 | 45 - 105 | U/L |
| Gamma glutamyl transpeptidase | 31 | 4 - 35 | U/L |
C reactive protein
Explanation:
This is an acute phase of protein produced predominantly by the liver in response to inflammatory cytokines.
Results
| Investigation Name | Investigation Result | Normal Range | Units |
|---|---|---|---|
| C reactive protein | 30 | < 10 | mg/L |
Full blood count
Rationale:
If the patient is anaemic it may suggest occult bleeding which would require further investigation and questioning. The presence of a low haemoglobin will heighten awareness to look out for further bleeding and limit the use of further anticoagulants such as heparin and powerful antiplatelet drugs.
Results & Explanation
| Investigation Name | Investigation Result | Normal Range | Units |
|---|---|---|---|
| Haemoglobin | 90 | 115-165 | g/L |
| White cell count | 10.1 | 4-11 | x109/L |
| Neutrophils | 6.8 | 1.5-7.0 | x109/L |
| Platelets | 350 | 150-400 | x109/L |
The results indicate the patient is anaemic. Any acute inflammatory event can cause an increase in the neutrophil count.
Chest X-ray
Rationale:
The chest X-ray is useful to document the examination findings of pulmonary oedema or in this case ARDS. In addition, there may be evidence of another cause of pain such as air under the diaphragm (viscus rupture) or aortic dissection/thoracic aortic aneurysm (widened mediastinum, pleural effusions).
Results & Explanation
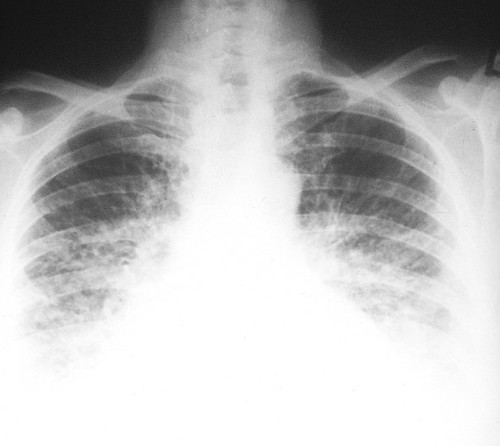
A ground glass appearance in the lower zones, with prominent upper lobe blood vessels, is typical of pulmonary oedema/ARDS.
FAST scan
Rationale:
FAST (Focussed Abdominal Sonography for Trauma) is a rapid non-invasive bedside test to detect the presence of free fluid within the abdomen. The extended-fast scan can also detect pleural effusions and a pneumothorax. The FAST protocol looks for fluid in Morison’s pouch, pericardium, splenorenal angle and in the pelvis. It also examines the aorta for AAA. In this scenario a positive finding would alert the clinician to the diagnosis of a leaking AAA.
Results & Explanation
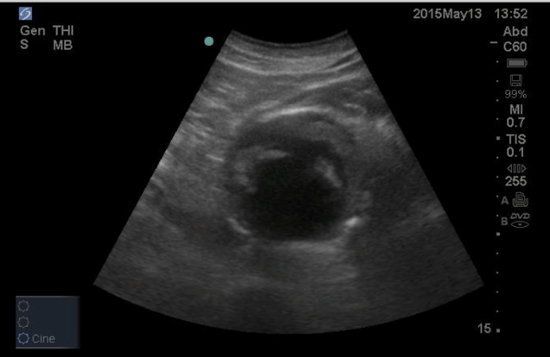
FAST scan detects an 8cm AAA
CT Angiogram of the Aorta
Rationale:
The presence of AAA on FAST would mean an immediate CTA should be performed. This is the gold standard for detecting a leaking AAA and can also identify the anatomy of the aneurysm so that the vascular surgeons can plan the repair.
Results & Explanation

The CTA identifies a leaking AAA of 8cm
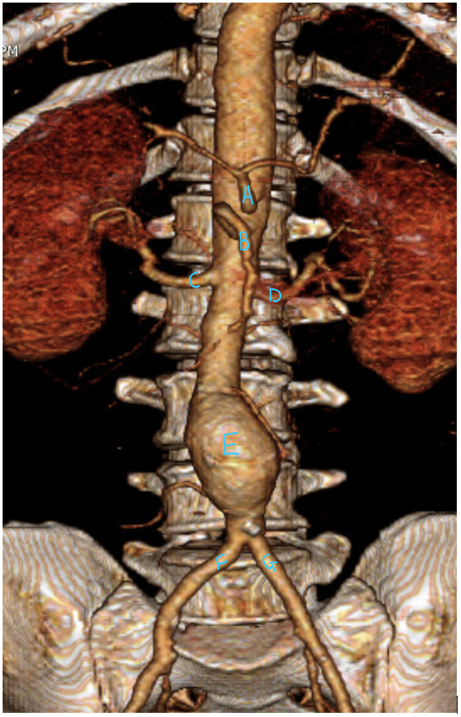
[SOURCE: Published with permission from LearningRadiology.com (annotated version of original).]
Labels for Figure 7
- A :
- Coeliac Artery
- B :
- Superior Mesenteric Artery
- C :
- Right Renal Artery
- D :
- Left Renal Artery
- E :
- Abdominal Aortic Aneurysm
- F :
- Right Common Iliac Artery
- G :
- Left Common Iliac Artery