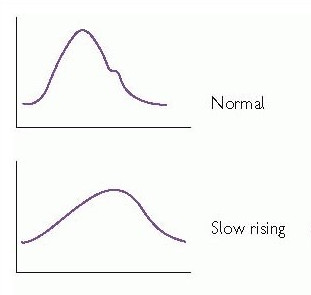
Low volume, slow-rising pulse and narrow pulse pressure
These findings result from prolonged left ventricular ejection through a narrowed aortic valve. This can be graphically presented as per Fig 1.
Left ventricular ejection through a narrowed aortic valve similary explains a heaving (also described as “sustained”) (pressure overloaded) apex beat, which is typically not displaced until late in the disease process when heart failure ensues.
Systolic crescendo-decrescendo murmur
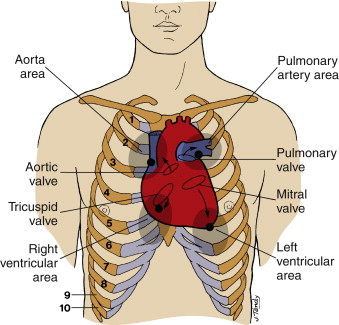
The murmur of aortic stenosis is best heard over the aortic area (right second intercostal space with radiation to the carotids; see Fig 2). It should be noted that radiation to the carotids is a sensitive finding in severe aortic stenosis and should therefore be routinely sought if aortic stenosis is suspected.
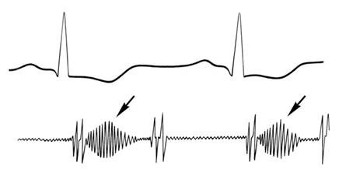
The murmur is mid- to high-pitched and starts shortly after the first heart sound and ends before the second heart sound, if this is still audible (Fig 3).
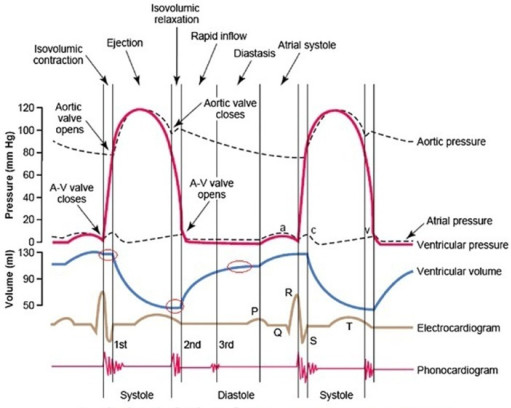
Because the second heart sound is predominantly generated by closure of the aortic valve, an immobile, stenotic valve typically causes a quiet or absent S2 (Fig 4).
Remember, it is important to always assess for other murmurs if you hear aortic stenosis as mixed valve disease with a common aetiology (rheumatic fever, for example) is a common finding.