Henry Smith
83, Male
Mr Smith’s diagnosis is severe calcific aortic stenosis.
Like many disease processes, aortic stenosis can be usefully described under the following headings:
Aortic stenosis
-
Definition:
Aortic stenosis is the obstruction of blood flow across the aortic valve. -
Epidemiology
It is Increasingly common, affecting 2-3% of people over the age of 65 and, untreated, severe aortic stenosis has a 4-year all-cause mortality of 81% among elderly patients (Pilgrim T et al Heart doi:10.1136/heartjnl-2014-306106).
Symptomatic aortic stenosis is more common in men.
-
Aetiology
Aortic stenosis has several causes, including congenital (including bicuspid aortic valve), acquired (calcific degeneration, rheumatic aortic valve disease) and sub- and supra-valvular obstruction (see Fig 7). By far the most common in Mr Smith’s age cohort is senile calcific degeneration (see Table 1).Age < 70 Age > 70 Bicuspid aortic valve (50%) Degenerative (48%) Postinflammatory (25%) Bicuspid (27%) Degenerative (18%) Postinflammatory (23%) Unicommisural (3%) Hypoplastic (2%) Hypoplastic (2%) Indeterminate (2%) Table 1. Aetiology of aortic stenosis (at surgery) according to age of presentation. 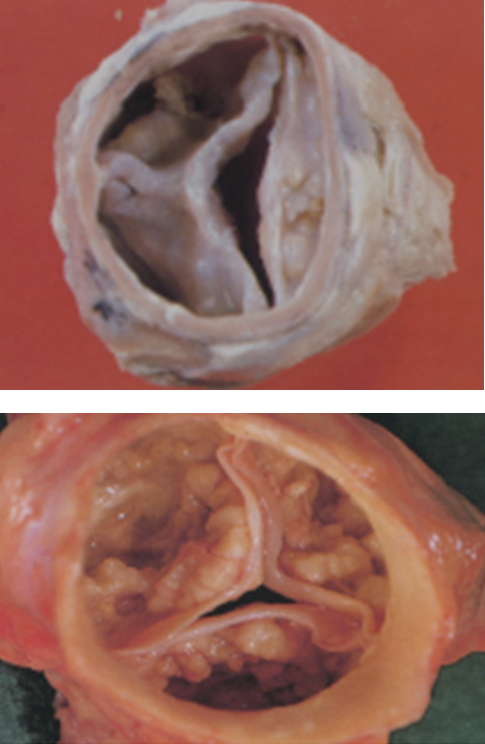
Fig 7. (A) Bicuspid aortic valve; (B) Degenerative calcific aortic stenosis. -
Pathophysiology
Aortic stenosis is typically caused by nodular fibrotic and calcific deposits on the aortic surface. As described, this results in increased left ventricular systolic pressure and ultimately heart failure. Furthermore, increased LV mass increases myocardial oxygen demand. Elevated diastolic pressure (LVEDP) exacerbates this by impairing the perfusion gradient so that demand can not be met and subendocardial ischaemia ensues. Patients experience this as angina and this is the probable explanation for Mr Smith’s chest tightness at peak exertion. -
Symptoms
Symptoms usually develop after an asymptomatic period of up to 20 years. The classic triad of symptoms is chest pain, heart failure and syncope (caused by cerebral hypoperfusion). -
Signs
As described in Patient Examination section.
In addition, an ejection click may be heard if the valve is bicuspid and, in severe aortic stenosis, a 4th heart sound (heard after atrial contraction and before S1, indicating forceful atrial contraction against a non-compliant ventricle) may be heard.
-
Investigations
As described in Investigations-Results section.
-
Management
As described in Patient Management section.
-
Prognosis
Untreated, aortic stenosis has a poor prognosis. Untreated, symptomatic patients with moderate-severe aortic stenosis have a higher mortality, estimated to be approximately 25% at 1 year and 50% at 2 years.
Conventional teaching dictates that mean survival from onset of symptoms is 2 years if the symptom is breathlessness, 3 years if it syncope and 5 years if it is angina. This is often demonstrated using Fig 8; however, there is a problem with this figure (can you spot it?).
Asymptomatic patients (regardless of the severity of aortic stenosis) have an excellent prognosis (<1% mortality per year). Predicting the rate of progression is difficult, and varies between patients, co-morbidities and aetiologies, but is estimated to be in the region of 0.1 to 0.3 cm2 valve area per year.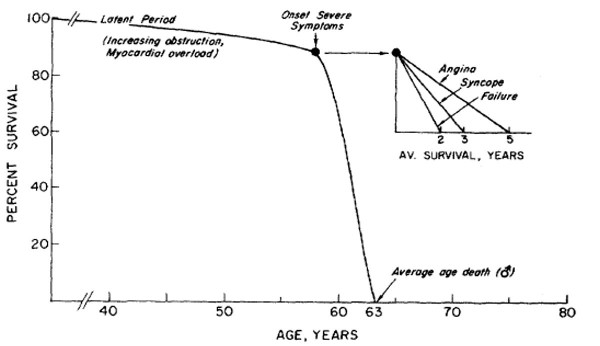
Fig 8. Commonly used graph to explain the prognosis in untreated aortic stenosis
(Circulation 38(Suppl V);61,1968)